B) Renal solid lesions:
Renal cell carcinoma:
-Is the most common solid or mixed lesion seen in the kidney.
-Any solid or cystic renal lesion should be considered a renal cell carcinoma until prove otherwise by biopsy.
-Staging of renal cell carcinoma
*Stage 1 : Tumor less 7 cms within the renal capsule.
*Stage 2 : Tumor more than 7 cms invading capsule but not gerota's fascia.
*Stage 3 : Renal vein invasion or lymph node invasion.
*Stage 4 : Tumor reaching beyond gerota's fascia or metastases to other organs.

 |
| Unenhanced (far left), corticomedullary phase (left middle), nephrographic phase (right middle), and excretory phase (far right) CT scans show a 1-cm low-attenuation mass (arrow) in the right renal cortex. The tumor is not clearly visible on the unenhanced and corticomedullary phase images; it is better demonstrated on the nephrographic and excretory phase images |
 |
| Cystic renal cell carcinoma ( with mural nodule). |
 |
| Contrast-enhanced transverse CT scan in an 86-year-old woman with a category IV lesion depicts a complex cystic mass with mural calcification (long arrow), wall enhancement, and obvious enhancing soft-tissue components (short arrow) adjacent to the wall (calcification score: 3). At surgery, this lesion was revealed to be a cystic renal cell carcinoma |
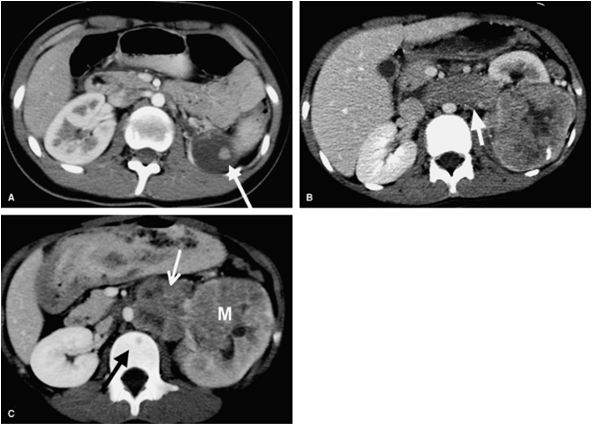 |
¨Renal cell carcinoma, spectrum of appearances. A: Contrast-enhanced CT scan in a 15-year-old girl demonstrates a cystic left renal mass (arrow) with a focal enhancing nodule (Bosniak IV lesion). The nodule makes it unlikely that this mass is a simple cyst. The cystic appearance resulted from necrosis. B: CT in a 12-year-old boy shows a large, heterogeneous soft tissue tumor extending exophytically from the kidney and invading the renal vein (arrow). C: CT in a 7-year-old boy shows a heterogeneous mass (M) replacing the upper pole of the left kidney, para-aortic adenopathy (white arrow), and a lytic bone metastasis ,black arrow |
-Golden rule:
¨To differentiate between simple renal cyst and renal cell carcinoma , you must do MRI for the case , if the lesion shows hypo intense in T1 and hyper intense in T2 while with contrast enhancement , it will reveal no enhancement ,so your diagnosis should be a simple renal cyst
¨While if MRI revealed enhancement of the wall , mural nodules or heterogenous enhancement , your diagnosis should be renal cell carcinoma
Another golden rule is that the presence of calcium in the wall of a renal cyst is suspicious for renal cell carcinoma by 25% incidence
Nephroblastoma or wilm's tumor
Occurs in children 1-5 years old
Bilaterality in 30% of cases
Common renal vein invasion and common deposits in the lung
Uncommon deposits in the liver and lymph nodes
Radiological appearance is similar to that of the renal cell carcinoma, so the only differential between both are the age of the patient, if it is child or adult, and also by site of secondaries if possible
 |
| Contrast-enhanced CT scan reveals fluid-attenuating material anteromedially, most likely hemorrhage, in the large heterogeneous mass. Linear calcification is present posteriorly |
Differential diagnosis of a low attenuated mass the renal parenchyma
Renal cyst
Acute pyelonephritis
Renal cell carcinoma or wilm's tumor according to edge
Lymphoma
Metastases
Look to the coming image below

Lymphoma
Multiple parenchymal renal masses usually have negative mass effect on the edge of kidney
Look at the spleen for further lesions and for retroperitoneal area for bulky lymph nodes
Usually seen in immuno compromised patient as in AID'S
 |
| Contrast enhanced CT image at the level of renal hila shows bilateral, smoothly enlarged kidneys showing a striated nephrogram. No focal lesions were identified |
Golden rule
¨Evidence of bilateral kidney diffuse enlargement with scanty area of secretory system enhancement suggest renal lymphoma
¨Lymphoma appears hypo echoic by ultrasound as a cystic lesion .In case of renal lymphoma , we can found diffuse hypo echogenecity of kidney
Transitional cell carcinoma
¨The most common tumor of renal pelvis
Multiple lesions in about 30%¨Diagnosed as a filling defect in pelvis
 |
| Transitional cell carcinoma seen as a filling defect in the left pelvis |
Benign renal lesions
Oncocytoma
No comments:
Post a Comment